
Disc Herniation: Everything You Need to Know
- staystrongtherapy
- Dec 5, 2025
- 16 min read
Updated: Jun 29
All information in this blog is supported by NICE guidelines and peer-reviewed research. Reference numbers appear throughout, the full list can be found at the bottom of the page.
What Is a Disc Herniation?
The term "slipped disc" is one of the most commonly used phrases in back pain, but it is actually a little misleading. Discs do not slip. They are firmly attached to the vertebrae above and below them and cannot move out of place. What actually happens is a gradual or sudden change in the structure of the disc itself, ranging from minor internal damage through to significant material escaping the disc and pressing on nearby nerves.
The pathophysiology of disc herniation is believed to be a combination of compression of the nerve by the displaced nucleus pulposus and a local increase in inflammatory chemical messengers known as chemokines. ¹ Understanding the different stages of this process helps explain why some people have mild discomfort whilst others experience severe pain, and why the right treatment approach can vary significantly depending on what stage you are at
The incidence of disc herniation is approximately 5 to 20 cases per 1,000 adults annually, is most common in people aged 30 to 50, and in 95% of cases the affected levels are L4-L5 and L5-S1, the lowest two levels of the lumbar spine. ¹
Understanding the Structure of Your Disc
Before looking at the stages, it helps to understand what a disc is made of. Each intervertebral disc, the cushioning structure between each pair of vertebrae,
has two main components:
The annulus fibrosus: a tough outer ring made of approximately 15 to 20 layers of criss-crossing collagen fibres, providing strength and containing the inner material under pressure. Think of it as the thick rubber wall of a car tyre.
The nucleus pulposus: a soft, gel-like centre that acts as the disc's shock absorber, distributing load evenly when you move, bend, or lift. Think of it as the pressurised air inside the tyre.
Discs have a very poor blood supply, which means they rely on movement and hydration to receive nutrients and remove waste products. This is one of the key reasons why staying active is so important for disc health and why prolonged inactivity or poor movement patterns can accelerate disc deterioration over time. ²
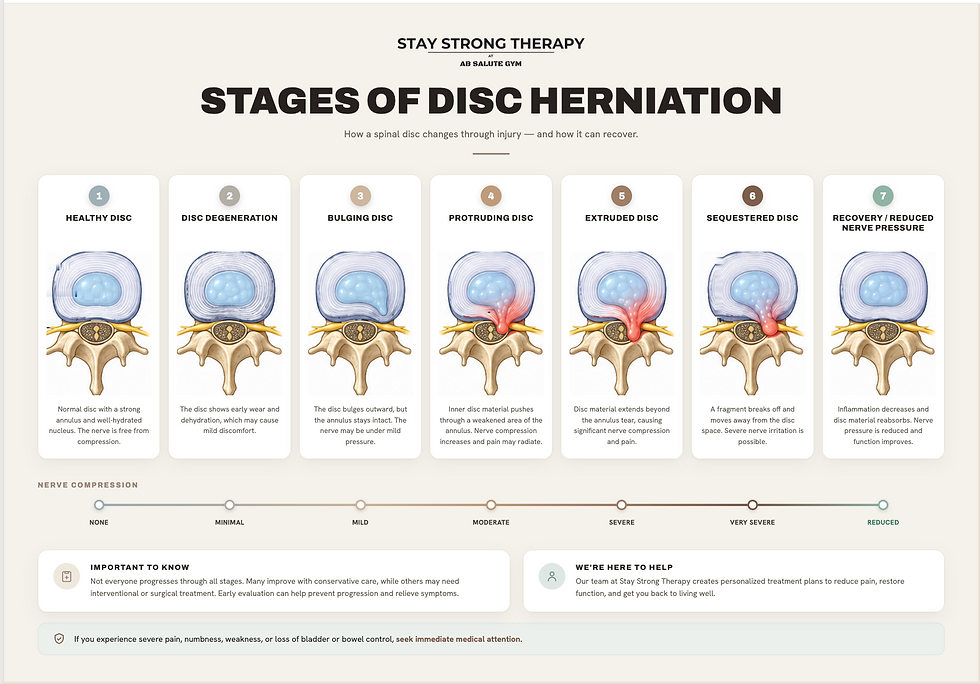
The Five Stages of Disc Herniation
Stage 1: Disc Degeneration
This is the earliest stage and is often the precursor to all subsequent changes. Over time, beginning as early as our late twenties, the discs begin to lose water content and become less hydrated and supple. The collagen fibres of the annulus can begin to show early signs of wear. The disc gradually loses height, becomes stiffer, and is less able to absorb and distribute load efficiently.
It is vital to understand that disc degeneration is a completely normal part of ageing. The findings of imaging studies are not necessarily correlated with the symptoms you are experiencing as degenerative disc changes are frequently visible on scans in people who have no pain at all. ² Many people have significant degeneration on an MRI scan and feel completely fine, whilst others with minimal changes experience significant pain. This is one of the key reasons why UK guidelines advise against routine imaging for back pain, a scan finding does not always reflect a person's experience. ³
Symptoms at this stage:
Often none at all
Occasional stiffness or mild aching in the lower back, particularly after prolonged sitting or inactivity
Discomfort that eases with gentle movement and warmth
What makes it worse: Prolonged sitting, inactivity, heavy or repetitive loading, dehydration, smoking
What helps: Regular movement, staying hydrated, gentle exercise, maintaining a healthy weight
Stage 2: Annular Fissure (Annular Tear)
As the disc degenerates and the annulus fibrosus comes under repeated stress, small tears or cracks can develop within its layers. These are called annular fissures (sometimes annular tears). They can occur gradually through wear, or more suddenly through a specific loading event such as heavy lifting or a twisting injury.
Most annular fissures produce no pain at all. However, some may be painful, particularly when the tear allows inflammatory chemicals contained within the nucleus to leak outward and irritate the surrounding structures or nearby nerve endings. Chronic pain from annular fissures can also occur due to the ingrowth of new nerve endings into the damaged area, which is usually seen near the dorsal root ganglion. ⁴
Think of this stage like a crack forming in the wall of a dam, the structure is compromised, but the water has not yet escaped. The fissure itself may heal partially with time and appropriate management, but because the disc has a poor blood supply, complete repair is limited. This is why early intervention and reducing provocative loading is important at this stage. ⁴
Symptoms at this stage:
Central lower back pain that can be sharp or aching
Pain that is worse with flexion (bending forward), prolonged sitting, or loading
Possible localised tenderness over the affected spinal level
Pain may refer into the buttock or thigh but typically does not travel below the knee at this stage
No neurological symptoms such as tingling, numbness, or leg weakness
What makes it worse: Bending forward, prolonged sitting, heavy lifting, twisting, coughing or sneezing
What helps: Gentle extension-based movement (such as standing up straight or lying on your front), heat, avoiding provocative loading, manual therapy, and keeping active within a comfortable range
Stage 3: Disc Bulge (Diffuse Bulge or Protrusion)
As fissures develop and the nucleus loses hydration, the disc can begin to bulge outward beyond its normal boundary. There are two distinct subtypes here that are important to understand:
Diffuse bulge: The presence of disc tissue extending beyond the edges of the ring apophyses throughout the circumference of the disc is called a bulge and is not considered a true form of herniation. It is a result of tears in the annulus fibrosus and can be seen as an adaptation to adjacent deformity or degeneration. ⁵ A diffuse bulge affects more than 25% of the disc circumference and represents general weakening of the outer wall rather than focal displacement of nuclear material.
Protrusion: A protrusion indicates that the base of the displaced disc material, where it connects to the disc, is wider than the displaced material itself, meaning the nuclear material is pushing outward but is still contained within the outer annular fibres. ⁵ Think of pressing your thumb into a water balloon; the balloon bulges outward at the point of pressure, but nothing has escaped.
At this stage, the disc material may begin to encroach on the spinal canal or the small openings through which nerve roots exit the spine, causing pain both from mechanical pressure and from the inflammatory response the disc generates. A posterolateral protrusion, the most common direction, usually compresses the nerve root at the next lower level, as the nerve crosses the level of the disc in its path to its exit point. ¹
Symptoms at this stage:
Lower back pain, often more significant than at earlier stages
Pain that may now begin to radiate into the buttock and back of the thigh
Pain that is noticeably worse when sitting, as sitting increases pressure on the lumbar discs by approximately 40% ⁶
Possible early tingling or mild numbness in the thigh if the nerve root is being irritated
Symptoms usually affect one side
Pain may ease when lying down with knees bent or when walking gently
What makes it worse: Sitting for prolonged periods, bending forward, coughing, sneezing, straining, lifting
What helps: Frequent position changes, extension-based movements such as walking or lying prone (on your front), gentle exercise, manual therapy to restore spinal movement and reduce nerve tension
Stage 4: Disc Extrusion
An extrusion represents a significant step up in severity from a protrusion. Extrusion is present when the disc material that has displaced is wider at its displaced point than at its base meaning it has broken through a defect in the outer annular fibres and, whilst it may still be connected to the main disc, it is no longer contained within the annulus. ⁵
Think of an extrusion like toothpaste being squeezed through a tear in the tube, the material has escaped through the breach but is still attached at the source. Once the annulus is torn and nucleus material extrudes, the disc becomes vulnerable to further damage, as these annular tears cannot heal spontaneously due to the disc's poor blood supply. ⁷
At this stage, two things are happening simultaneously to the nerve root: mechanical compression from the displaced disc material pressing on it, and a significant chemical inflammatory response. Research has confirmed that inflammatory cytokines and chemical mediators, including interleukins IL-1β, IL-6, IL-8, and TNF-α, are released from the herniated disc material and can directly sensitise and irritate the nerve root even in the absence of significant physical compression. ⁸ This is why some people with extruded discs have profound leg pain from a relatively small amount of physical compression, the chemical irritation is a major driver of their symptoms.
Importantly, extruded discs have the highest rate of spontaneous reabsorption of any stage. Research has shown that disc morphology is a significant predictor of spontaneous regression, with extruded discs having a higher likelihood of natural reabsorption than protrusions or bulges. ⁹ The body recognises the extruded disc material as foreign and mounts an immune response, macrophages (the body's clean-up cells) infiltrate the area and gradually break down and reabsorb the disc material over weeks to months. This is one of the most clinically important and reassuring findings in modern spine research. ⁹
Symptoms at this stage:
Significant leg pain, often more severe than the back pain itself, travelling below the knee into the calf, foot, or toes
Sharp, burning, shooting, or electric-shock quality pain
Tingling or pins and needles along a specific strip of the leg or foot
Possible numbness or reduced sensation in the leg or foot
Possible weakness in the leg, foot, or toes
Symptoms significantly worse when sitting, bending forward, coughing, or sneezing
Some relief when lying down with knees bent or when walking — movement can temporarily reduce nerve compression
What makes it worse: Sitting, sustained lumbar flexion (bending forward), coughing, sneezing, heavy loading
What helps: Gentle walking, extension-based positions, nerve mobilisation exercises (nerve flossing), manual therapy, medical acupuncture, and consistent gentle activity. NICE guidelines recommend staying as active as possible and beginning appropriate conservative treatment early. ³
Stage 5: Sequestration (Free Fragment)
Sequestration is the most advanced stage of disc herniation. Sequestration indicates that the displaced disc material has completely lost continuity with the parent disc, it is a free fragment floating within the spinal canal, no longer attached to the disc it came from. ⁵ The fragment may migrate upward or downward within the canal, and depending on where it settles, can compress one or more nerve roots.
Paradoxically, whilst sequestration sounds alarming, it can also be the stage at which the body mounts the most vigorous immune response, meaning spontaneous reabsorption is possible, and many cases do improve without surgery. Systematic review evidence shows that extruded and sequestered disc fragments have higher rates of spontaneous reabsorption than contained herniations, likely because the free fragment is more exposed to the vascular and immune environment of the spinal canal, triggering a stronger macrophage-driven clearance response. ⁹
However, sequestration carries a higher risk of significant neurological compromise if the free fragment compresses critical nerve structures, and close monitoring is essential. NICE guidelines are clear that red flag symptoms, particularly any signs of cauda equina syndrome, require urgent medical assessment. ³
Symptoms at this stage:
Severe, often debilitating leg pain
Significant neurological symptoms including numbness, tingling, and weakness
Possible foot drop (difficulty lifting the foot) if the nerve to the foot is significantly compressed
Symptoms may affect both legs in rare cases if the fragment is large and central
Any loss of bladder or bowel control, or numbness in the saddle area (inner thighs and groin), requires immediate attendance at A&E, this may indicate cauda equina syndrome, which is a medical emergency ³
What to Look Out For
UK guidelines advise seeking urgent medical attention if any of the following are present, as they may indicate cauda equina syndrome or another serious condition: ³
Loss of bladder or bowel control
Numbness or tingling in the inner thighs, groin, or saddle area
Rapidly worsening weakness in both legs
Severe pain not relieved by any position, particularly at night
Back pain following significant trauma
Unexplained weight loss alongside back pain
The Good News: Most Disc Herniations Improve Without Surgery
One of the most important and reassuring messages from modern research is that the majority of disc herniations, even significant ones, do not require surgery and will improve with the right conservative management. ¹⁰
Studies have found that some disc herniation patients, without undergoing surgery, experience spontaneous shrinkage and reabsorption of the disc tissue along with relief of back and leg pain, a phenomenon referred to as LDH reabsorption. Research suggests this reabsorption process is closely related to inflammatory responses, macrophage activation, extracellular matrix enzyme balance, and neovascularisation. ⁹
Both surgical and conservative treatments for lumbar disc herniation result in similar clinical outcomes over mid-term and long-term follow-up periods, with conservative treatment carrying a lower risk of complications than surgery and being favoured by most patients. ¹⁰
Myths vs Facts
"I need surgery to fix my disc." The vast majority of disc herniations; including extruded discs, improve with conservative care. Surgery is generally reserved for cases with significant and worsening neurological deficit, or where conservative treatment has failed over a sustained period. ¹⁰
"A scan showing a herniated disc means I will always have pain." Not at all. Many people have disc herniations visible on MRI with no pain whatsoever. The disc can reabsorb over time, and symptoms often resolve long before the disc fully returns to normal on imaging. ²
"I should rest and not move until it heals." UK guidelines advise against prolonged rest. Staying gently active, within a comfortable range, promotes healing, maintains muscle strength, reduces nerve sensitivity, and leads to better outcomes than inactivity. ³
"If I have a herniated disc, I will need to be careful for the rest of my life." With appropriate rehabilitation and the right movement habits, the majority of people who experience disc herniation return to full normal activity, including sport, manual work, and exercise. ¹⁰
How We Can Help
At our clinic, all treatments are delivered in line with UK guidelines and current research evidence. For disc herniation, we take a multimodal approach, combining treatments to address pain, inflammation, nerve sensitivity, and movement dysfunction simultaneously. This is consistently shown to produce better outcomes than single-treatment approaches. ¹⁰
Osteopathic manual techniques and spinal manipulation / mobilisation: UK guidelines recommend manual therapy; including spinal manipulation, mobilisation, and soft tissue techniques, as part of a treatment package for low back pain and sciatica. ³
For disc herniation specifically, manual therapy aims to restore movement to restricted spinal joints, reduce compressive loading on the affected disc level, and improve the mechanics of the surrounding structures.
Deep tissue and sports massage: Soft tissue massage is recognised by NICE as a component of manual therapy for back pain. ³ For disc herniation, targeted massage reduces paraspinal muscle spasm, which often develops as a protective response around an irritated disc, improves circulation, and reduces the secondary muscle tension that can worsen nerve compression and pain.
Medical acupuncture: We use medical acupuncture as part of a broader, multimodal treatment plan. Research has shown that acupuncture significantly reduced leg pain and improved functional disability scores in people with chronic sciatica from disc herniation. ¹² ¹³
Whilst current UK guidance does not recommend acupuncture as a standalone treatment, the growing body of high-quality research supports its use within a multimodal plan, and we are transparent about this distinction.
Exercise and Rehabilitation
Exercise is one of the most powerful tools in the management of disc herniation and is recommended at every stage of recovery by UK guidelines. ³ Research has found that exercise therapy significantly enhanced core muscle strength and lumbar stability, relieved lower back and leg pain, and improved quality of life in people with lumbar disc herniation. ¹⁵
In the early, acute stage:
Gentle walking is one of the most beneficial things you can do: even short distances help
Avoid prolonged sitting: get up and change position frequently
Avoid sustained forward bending, which increases pressure on the disc
Gentle lying prone (on your front) can help centralise symptoms. If it relieves your leg pain and brings it closer to your back, this is a positive sign
As symptoms begin to settle:
Extension in lying: lying on your front and gently propping up on your forearms, or pressing up onto your hands. This is the foundation of the McKenzie approach and is particularly effective for disc-related pain with leg symptoms, as it encourages the disc material to move away from the nerve. Your practitioner will advise if this is appropriate for your presentation.
Knee-to-chest stretch: gently drawing one knee toward your chest lying on your back to reduce pressure on the affected nerve root
Pelvic tilts: activates the deep spinal stabilisers without loading the disc
Piriformis stretch: lying on your back, crossing one ankle over the opposite knee and gently drawing the thigh toward you
Longer-term rehabilitation:
Core stabilisation exercises: bird-dog, dead bug, and plank progressions as they help to protect the spine and reduce recurrence risk ¹⁵
Sciatic nerve glide: sitting upright, slowly straightening one knee and gently flexing the foot up and down. This mobilises the sciatic nerve through surrounding tissues and reduces neural tension
Gradual return to walking, swimming, and low-impact exercise
Pilates-based rehabilitation has good evidence for disc-related back pain ¹⁵
Progressive strengthening of the glutes, hips, and legs reduces the load placed on the lumbar spine during daily activities
Always work within a comfortable range. An increase in back pain during exercise is generally acceptable (max 4 out of 10 pain); an increase in leg pain, tingling, or numbness is a signal to ease off and seek guidance. We will design a programme appropriate to your specific stage and presentation.
Living With a Disc Herniation: Practical Day-to-Day Tips
UK guidelines emphasise the importance of self-management advice at every stage of care. ³ Here are practical tips for managing day to day:
Sitting: This is the position most likely to aggravate disc herniation. Avoid sitting for more than 20 to 30 minutes without standing and moving. Use a lumbar support or rolled towel in the small of your back. Consider a slightly reclined seating position; this reduces lumbar disc pressure compared to sitting bolt upright or slumped.
Standing and walking: Generally much better tolerated than sitting. Stand where possible, and use a small footstool to alternate resting one foot at a time if standing for extended periods.
Sleeping: Most people find lying on their side with a pillow between the knees most comfortable, as this reduces rotational stress on the lower spine. Lying on your back with a pillow under your knees can also help. Avoid sleeping on your front if it increases leg pain.
Lifting: Avoid lifting wherever possible during the acute phase. When you must lift, keep the load close to your body, bend at the knees, and avoid twisting at the same time as lifting.
Driving: Driving places significant compressive load on the lumbar discs due to vibration and sustained sitting. Take regular breaks, use a lumbar support, and avoid long journeys in the acute stage where possible.
Work: If you work at a desk, a sit-stand desk is ideal. If not, set reminders to stand and walk every 20 to 30 minutes. If your work involves manual labour, discuss a phased return with your practitioner.
Heat: Applying warmth to the lower back can help ease surrounding muscle spasm and improve comfort, particularly in the morning.
What to Expect at Your First Appointment
At your first appointment, we will take a thorough case history to understand how your symptoms started, which stage and type of disc herniation we are likely dealing with, and how your symptoms are behaving, in particular, whether movement centralises or peripheralises your pain (brings it closer to your back or pushes it further into your leg), which is a key indicator that guides treatment. We will carry out a full neurological and orthopaedic assessment and design a personalised, evidence-based treatment plan in line with NICE guidelines. ³ You will always be fully informed about your condition in plain language and will never be rushed.
Realistic Recovery Timelines
Recovery timelines vary depending on the stage and severity of the herniation, how long symptoms have been present, and how quickly treatment begins. As a general guide:
Acute disc bulge or protrusion: Many people see significant improvement within 4 to 8 weeks with appropriate conservative care ¹⁰
Disc extrusion with sciatica: Most cases see meaningful improvement within 6 to 12 weeks. Around 90% of cases improve with conservative care over 12 weeks ¹⁵
Sequestration: Recovery timelines are more variable and depend on the size and position of the free fragment. Many cases still resolve conservatively, though the process may take several months and requires careful monitoring
Starting treatment early, staying active, and engaging with rehabilitation exercises consistently are the factors most associated with faster recovery. ¹⁰
Frequently Asked Questions
Do I need an MRI scan?In most cases, NICE guidelines advise against routine imaging. A thorough clinical assessment is usually sufficient to guide treatment. Your practitioner will advise if a referral for imaging is appropriate — for example, if symptoms are severe, worsening, or failing to respond to treatment. ³
Can a disc herniation heal on its own?Yes — in many cases it can. The body has a remarkable ability to reabsorb disc material over time, particularly at the extrusion and sequestration stages. Conservative treatment supports and accelerates this natural process. ⁹
Can I exercise with a disc herniation?Yes — with guidance. Appropriate exercise is one of the most important things you can do. The key is working within the right range for your stage and presentation, which your practitioner will help you establish. ³ ¹⁵
Will this happen again?Recurrence is possible, particularly if underlying factors such as core weakness, movement habits, and posture are not addressed. This is why rehabilitation is such a central part of your care with us.
Ready to take the first step toward recovery? Get in touch using the contact form and we will help you find the right treatment for your disc herniation.
References
Physiopedia. Disc Herniation. Available at: https://www.physio-pedia.com/Disc_Herniation
The Diagnosis and Treatment of Degenerative Changes of the Lumbar Spine. Deutsches Arzteblatt International. PMC. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC12516344/
National Institute for Health and Care Excellence (NICE). Low Back Pain and Sciatica in Over 16s: Assessment and Management. NICE Guideline [NG59]. Published November 2016, last updated December 2020. Available at: https://www.nice.org.uk/guidance/ng59
Dydyk AM, Ngnitewe Massa R, Mesfin FB. Disc Herniation. In: StatPearls. StatPearls Publishing. Updated August 2023. Available at: https://www.ncbi.nlm.nih.gov/books/NBK560878/
Fardon DF, et al. Lumbar Disc Nomenclature: Version 2.0. Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Radiology Assistant Summary. Available at: https://radiologyassistant.nl/neuroradiology/spine/lumbar-disc-nomenclature-2-0
Wilke HJ, et al. New in vivo measurements of pressures in the intervertebral disc in daily life. Spine. 1999. Referenced in: StatPearls Lumbar Disc Herniation. Available at: https://www.ncbi.nlm.nih.gov/books/NBK560878/
Spine Surgery Insights. Extrusion Disc Herniation: Causes, Symptoms and Treatment Options. 2025. Available at: https://www.spine.md/insights/extrusion-disc-herniation
Budrovac D, et al. Biological Mechanisms of Pain Management in Lumbar Disk Herniation: Focus on Cytokine Correlations and Therapeutic Approaches. International Journal of Molecular Sciences. 2025. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12652388/
Rashed S, Vassiliou A, Starup-Hansen J, Tsang K. Systematic review and meta-analysis of predictive factors for spontaneous regression in lumbar disc herniation. Journal of Neurosurgery: Spine. 2023;39(4):471-478. Available at: https://pubmed.ncbi.nlm.nih.gov/37486886/
Harding T, et al. Exercise, manipulation and traction physiotherapy in the conservative management of lumbar disc herniation: A systematic review and meta-analysis. PMC. 2024. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC12595123/
Shi F, et al. Comparative clinical efficacy of acupuncture combined with manipulation and other non-pharmacological interventions in the treatment of lumbar disc herniation: a prospective, multi-arm, randomized, open-label, blinded endpoint trial. Frontiers in Medicine. 2025. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11738951/
Qu Z, Ju J, Qin H, Ding Y, Peng L. Effectiveness of acupuncture in the treatment of chronic sciatica from herniated discs: a systematic review and meta-analysis. Frontiers in Medicine. 2026. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12872920/
Tu JF, Shi GX, Yan SY, et al. Acupuncture vs sham acupuncture for chronic sciatica from herniated disc: a randomized clinical trial. JAMA Internal Medicine. 2024;184:1417-1424. Available at: https://doi.org/10.1001/jamainternmed.2024.5463
Cao H, et al. Update evidence of effectiveness on pain relieving of cupping therapy: a systematic review and meta-analysis of randomized controlled trials. Journal of Traditional Chinese Medicine. 2025;45(2):234-253. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11955767/
Du X, et al. Clinical efficacy of exercise therapy for lumbar disc herniation: a systematic review and meta-analysis of randomized controlled trials. Frontiers in Medicine. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11985520/
Figures:
Alessi J. Rehab services for herniated disc, lower back pain and sciatica. Personal Training Master. Published March 2023, last updated April 2026. Available at: https://www.personaltrainingmaster.co.uk/rehab-services-for-herniated-disc-lower-back-pain-and-sciatica/



Comments