
Sciatica: Do I Actually Have It?
- staystrongtherapy
- Jun 27
- 13 min read
All information in this blog is supported by NICE guidelines and peer-reviewed research. Reference numbers appear throughout, the full list can be found at the bottom of the page.
What Is Sciatica?
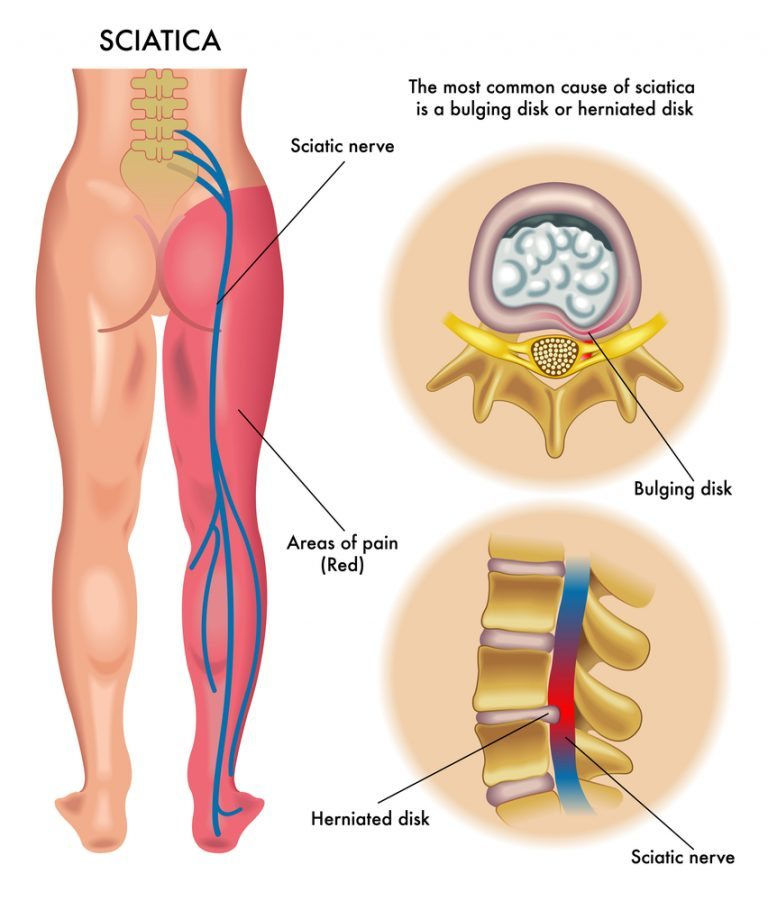
Sciatica is a term that gets used a lot, and quite often incorrectly. It describes pain that travels along the path of the sciatic nerve, which runs from the lower spine, through the buttock, and all the way down the back of the leg to the foot. True sciatica is caused by irritation or compression of one of the nerve roots that form the sciatic nerve, and it produces a very specific pattern of symptoms. ¹
Understanding what sciatica actually is, and what it is not, is one of the most important steps toward getting the right treatment.
True Sciatica vs Referred Pain: What Is the Difference?
This is something that causes a great deal of confusion, so let us break it down clearly.
What Sciatica Is NOT...
Many people experience lower back pain that spreads into the buttock and travels partway down the back of the thigh, sometimes reaching the back of the knee, but no further. This is known as non-specific low back pain with leg referral (aka somatic referral pain), and whilst it can be uncomfortable and feel alarming, it is not true sciatica.
Think of it this way: the joints, muscles, and discs of your lower back share overlapping nerve pathways with parts of your buttock and thigh. When these structures become irritated or inflamed, the brain can interpret that pain as coming from the leg, much like how a heart attack can cause pain in the left arm. The pain does not travel because a nerve is being compressed; it travels because the brain is misreading signals.
Typical pattern of somatic referred pain:
Dull, aching, or cramping sensation
Spreads into the buttock and back of the thigh
Stops at or above the back of the knee
No tingling, numbness, or weakness in the lower leg or foot
No pins and needles
This type of pain responds very well to manual therapy, massage, and exercise, and the outlook is generally very good. ²
If you are experiancing this type of pain referral, take a look at the Low Back Pain blog
What TRUE Sciatica Is
True sciatica, (aka lumbar radiculopathy), occurs when a nerve root in the lower spine becomes compressed or irritated, sending pain signals along the full length of that nerve. ³
Sciatica is characterised by radiating pain that follows a dermatomal pattern, a strip of skin supplied by a specific nerve root, and patients may also report sensory symptoms such as tingling, numbness, or pins and needles. ³
Typical pattern of true sciatica:
Sharp, shooting, burning, or electric-shock type pain
Travels from the lower back or buttock all the way down the leg; usually below the knee and often into the calf, foot, or toes
Tingling, numbness, or pins and needles in the leg or foot
Possible weakness in the leg, foot, or toes
Symptoms usually affect one leg only, though both can be involved in rare cases
Low back pain may be present but is often less severe than the leg pain ³
The annual prevalence of true sciatica ( aka lumbar radicular syndrome) in the general population, described as low back pain with leg pain travelling below the knee, varies from 9.9% to 25%. ¹
Other Things That Can Mimic Sciatica
It is also worth knowing that not everything that causes leg pain is coming from the spine. Several other conditions can produce similar symptoms and are sometimes mistaken for sciatica:
Piriformis syndrome: the piriformis muscle in the buttock sits very close to the sciatic nerve. If this muscle becomes tight or goes into spasm, it can compress the sciatic nerve directly, producing pain and tingling down the leg without any spinal disc involvement. This is sometimes called "wallet sciatica" and responds very well to targeted muscle release and stretching.
Sacroiliac joint dysfunction: the joint connecting your pelvis to your spine can refer pain into the buttock and sometimes the thigh, mimicking early sciatica.
Facet joint referral: inflamed facet joints in the lower back can refer pain into the buttock and thigh, usually above the knee.
Getting an accurate diagnosis is key, as the cause of your symptoms will determine which treatment approach is most appropriate. ⁴
What Is Causing the Nerve to Be Compressed?
Lumbosacral radiculopathy is typically caused by nerve root compression, most often due to intervertebral disc herniation, bony irregularities such as osteoarthritic bone spurs, or spinal stenosis; a narrowing of the spinal canal. ³
The most common cause is a herniated disc (sometimes called a slipped or bulging disc). The discs between your vertebrae act like shock absorbers. Each one has a tough outer ring and a soft gel-like centre. If the outer ring weakens or tears through injury, repeated strain, or simply wear over time, the soft inner material can push outward and press against a nearby nerve. Think of squeezing a jam doughnut: the filling pushes out under pressure.
Sciatica usually arises from lumbar nerve root compression or irritation, which is most often caused by disc protrusion or narrowing of the spinal canal, and may be associated with radicular pain and neurological deficits including muscle weakness, sensory disturbance, or altered reflexes. ³
The most commonly affected levels in the lumbar spine are L4-L5 and L5-S1, which is why symptoms most often travel into the back of the thigh, calf, and foot.
Common Signs & Symptoms
In line with NICE guideline NG59, the following symptoms are characteristic of sciatica: ¹
Shooting, burning, or electric pain travelling from the lower back or buttock down one leg, below the knee
Tingling or pins and needles in the leg, foot, or toes
Numbness or reduced sensation along the leg or foot
Weakness in the leg, foot, or toes with difficulty lifting the foot (foot drop) in more severe cases
Pain that is often worse when sitting, coughing, sneezing, or straining
Pain that may ease slightly when walking or lying down with the knees bent
Low back pain that is usually less severe than the leg pain itself ³
Symptoms to Look Out For:
UK guidelines advise that the following symptoms require urgent medical assessment, as they may indicate a serious condition called cauda equina syndrome, where the nerves at the base of the spine are severely compressed. This is a medical emergency. ¹
Please seek urgent medical attention or go to A&E immediately if you experience:
Loss of bladder or bowel control, or difficulty passing urine
Numbness or tingling in your inner thighs, groin, or saddle area (the area that would touch a saddle when sitting)
Sudden severe weakness in both legs
Sciatica that is rapidly getting worse on both sides
For non-emergency concerns, see your GP if your sciatica is severe, not improving after several weeks, or significantly affecting your daily life.
Realistic Healing Timelines: What to Expect
One of the most common questions people have is: how long will this last? The honest answer is that it varies, but the research gives us a helpful picture. ⁵
Acute sciatica (symptoms present for less than 6 weeks): Most people with acute sciatica see significant improvement within the first few weeks. About 90% of acute sciatica cases will resolve within 12 weeks with appropriate conservative care. ⁵ Many patients with sciatica recover within 6 weeks with conservative care, though this depends heavily on what is causing the nerve compression; a mild herniated disc may settle relatively quickly as inflammation decreases, while more significant structural problems may take longer. ⁵
Subacute sciatica (6–12 weeks):Symptoms may still be present but are usually improving. This is the stage where structured rehabilitation, manual therapy, and targeted exercise become especially important. Early, active treatment during this phase significantly reduces the risk of symptoms becoming chronic (long term). ⁶
Chronic sciatica (symptoms lasting longer than 12 weeks):Around 30-40% of sciatica patients continue to have symptoms for 12 months or longer. ⁵ This does not mean recovery is impossible, many people with chronic sciatica do improve significantly with the right multimodal treatment approach, which is why seeking professional help sooner rather than later matters.
Factors that influence your recovery timeline:
The underlying cause: disc herniation tends to improve as the disc material can reabsorb over time; spinal stenosis may be slower
How quickly treatment begins: early active management leads to shorter recovery times ⁶
Staying active: people who remain as mobile as possible tend to recover faster than those who rest completely
Overall health: conditions such as diabetes or obesity can slow nerve healing
Around 80 to 90% of sciatica cases caused by a herniated disc improve with conservative care over the long term, and surgery is only required in a small minority of cases. ⁵
Myths vs Facts
"Sciatica means I have a serious back problem." Not necessarily. The majority of sciatica cases resolve well with conservative, non-surgical treatment. Most are caused by disc herniation that the body is capable of healing over time. ⁵
"I need a scan to diagnose sciatica." UK guidelines advise against routine imaging for low back pain and sciatica in most cases, as scans frequently show changes that are normal with age and are not always the cause of symptoms. A thorough clinical assessment is usually sufficient. ¹
"I should rest completely until it passes." Prolonged rest is not recommended. Staying as gently active as possible and beginning appropriate treatment early leads to faster recovery. ¹ ⁶
"My pain goes to the back of my knee so I must have sciatica." Not necessarily, as explained above, pain that stops above or at the back of the knee is more likely to be somatic referred pain from the lower back, not true sciatica. A proper assessment will clarify this. ²
How We Can Help
At our clinic, all treatments are delivered in line with NICE guidelines NG59 and are supported by current research. We offer a multimodal approach; meaning we combine therapies rather than relying on a single technique, which the evidence consistently shows produces the best outcomes for sciatica. ⁶
Osteopathic manual techniques and spinal manipulation / mobilisation: UK guidelines recommend considering manual therapy, including spinal mobilisation, and soft tissue techniques, for managing low back pain and sciatica, as part of a treatment package that includes exercise. ¹ Our hands-on techniques are used to decompress irritated nerve roots, restore spinal joint mobility, and reduce muscle tension around the affected area. A 2021 systematic review of manual therapy for lumbar radiculopathy found encouraging evidence for pain reduction and functional improvement across a range of manual techniques. ⁷ nih
Neural mobilisation (nerve flossing): This is a gentle technique used to improve the mobility of the sciatic nerve through the surrounding tissues, helping to reduce tension, improve nerve conduction, and ease pain. Research suggests that neural mobilisation significantly reduced pain and disability in patients with lumbar radiculopathy. ⁸
Deep tissue and sports massage: We use targeted massage to release tight muscles, particularly in the lower back, gluteal region, and piriformis that may be contributing to nerve compression or irritation.
Medical acupuncture: We use medical acupuncture as part of a broader multimodal treatment plan alongside exercise and manual therapy. Research has found that acupuncture significantly reduced leg pain scores (1-10 pain scale) in people with chronic sciatica from disc herniation. ⁹ Whilst current UK guidance does not recommend acupuncture as a standalone treatment, the growing body of research supports its use within a multimodal plan, and we are transparent about this distinction.
Cupping and gua sha: We use these as complementary tools within a broader treatment plan. Current UK guidelines do not specifically address cupping or gua sha for sciatica; however, the available research supports their use as part of a combined approach to reducing muscle tension, improving circulation, and supporting recovery. ¹⁰
Exercise & Rehabilitation
Exercise is a central pillar of sciatica management. ¹ Exercise therapy can help to enhance core muscle strength and lumbar stability, which therefore relieves lower back and leg pain, and improves quality of life in people with lumbar disc herniation and associated nerve pain. ¹¹
In the early stages:
Gentle walking is one of the best things you can do, even short distances help
Avoid prolonged sitting or lying in one position, change position regularly
Do not push through severe leg pain; work within a comfortable range
As symptoms settle, begin gentle exercise:
Knee-to-chest stretch: lying on your back, gently draw one knee toward your chest and hold for 20–30 seconds. This can reduce pressure on the affected nerve root.
Pelvic tilts: lying on your back with knees bent, gently flatten your lower back to the floor. Activates deep spinal stabilisers without loading the disc.
Piriformis stretch: lying on your back with knees bent, cross one ankle over the opposite knee and gently pull the thigh toward you. This targets the piriformis muscle, which frequently contributes to sciatic pain.
Cat-cow stretch: gentle spinal mobilisation on all fours to maintain movement and reduce stiffness.
As you progress:
Core stabilisation exercises such as bird-dog and dead bug are essential for protecting the spine long term ¹¹
Gradually build up walking distance and introduce low-impact activities such as swimming
McKenzie exercises (repeated extension in lying) are often helpful for disc-related sciatica, we will guide you on whether these are appropriate for your presentation
Sciatic nerve glide (nerve flossing): sitting upright, slowly straighten one knee and gently flex your foot up and down. This helps mobilise the sciatic nerve through the surrounding tissues. Stop if this significantly increases leg pain. Again, we will guide you on whether this is appropriate for your presentation
Always work within a comfortable range. Aim to working within a 4 out of 10 on the pain scale. An increase in back pain during exercise is generally acceptable; an increase in leg pain, tingling, or numbness is a signal to ease off and seek guidance from us. ¹
Living With Sciatica: Practical Day-to-Day Tips
UK guidelines emphasise the importance of self-management advice at every stage of treatment. ¹ Here are practical tips to help manage your symptoms day to day:
Sitting: Avoid sitting for prolonged periods: get up and move every 20 to 30 minutes. Sitting increases pressure on the lumbar discs and can aggravate sciatica significantly. Try a rolled towel or lumbar support in the small of your back when seated.
Sleeping: Many people with sciatica find lying on their side with a pillow between their knees most comfortable, as this reduces pressure on the lower spine and nerve roots. Lying on your back with a pillow under your knees can also help.
Standing and walking: Walking is generally better tolerated than sitting or standing still. Wear supportive footwear and avoid standing in one position for long periods.
Driving: Take regular breaks and use a lumbar support. Try to keep your seat adjusted so your knees are roughly level with your hips.
Heat and ice: Applying heat to the lower back and buttock can help ease muscle spasm around the irritated nerve. Some people find ice more helpful in the acute phase to reduce inflammation. Try both and see what works for you.
Avoid heavy lifting: If you must lift, bend at the knees, keep the load close, and avoid twisting. This reduces pressure on the lumbar discs.
Avoid prolonged bending forward: Activities that load the lumbar disc in a flexed position; such as prolonged sitting, gardening, or leaning over a desk can worsen disc-related sciatica.
What to Expect at Your First Appointment
At your first appointment, we will take a full case history to understand exactly where your pain is travelling, how it started, what makes it better or worse, and how it is affecting your life. We will carry out a thorough neurological and orthopaedic assessment — including nerve tension tests such as the straight leg raise — to help us establish whether you have true sciatica, referred pain, or another contributing condition. In line with NICE guidelines, we will then discuss a personalised, evidence-based treatment plan with you. ¹
Frequently Asked Questions
Do I need an MRI scan? In most cases, NICE guidelines advise against routine imaging for sciatica. A clinical assessment is usually sufficient to guide treatment. Your practitioner will advise you if a referral for imaging is appropriate, for example, if your symptoms are severe, worsening rapidly, or not responding to treatment. ¹
How many sessions will I need? This varies depending on the cause, severity, and duration of your symptoms. Many people notice meaningful improvement within three to six sessions, particularly when early active treatment is combined with home exercises.
Will I need surgery? Surgery is rarely necessary. The vast majority, around 80 to 90% of sciatica cases caused by a herniated disc improve with conservative care over the long term, with surgery required in only a small minority of cases. ⁵ If your symptoms are severe and not responding to conservative treatment after several weeks, your practitioner will discuss referral options with you. clinicaltrials
Can sciatica come back?Yes, recurrence is possible, particularly if the underlying causes such as core weakness, posture, or movement habits are not addressed. This is why rehabilitation and exercise form a core part of your treatment plan.
Ready to get started? Get in touch with us today using the contact form and we will help you find the right treatment for your sciatica. Or simply book an appointment by clicking the button below
Lower Back Pain: References
National Institute for Health and Care Excellence (NICE). Low Back Pain and Sciatica in Over 16s: Assessment and Management. NICE Guideline [NG59]. Published November 2016, last updated December 2020. https://www.nice.org.uk/guidance/ng59
Corp N, et al. Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines. European Journal of Pain. 2021;25(3):585-601. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7839780/
Li Y, et al. Exercise intervention for patients with chronic low back pain: a systematic review and network meta-analysis. Frontiers in Public Health. 2023. https://pubmed.ncbi.nlm.nih.gov/38035307/
Zhai H, et al. Effectiveness of Physical Activity in the Management of Nonspecific Low Back Pain: A Systematic Review. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11678838/
Rubinstein SM, et al. Exercise Therapy Versus Manual Therapy for the Management of Pain Intensity, Disability, and Physical Function in People With Chronic Low Back Pain: A Systematic Review With Meta-Analysis and Meta-Regression. 2024-2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314856/
Mak S, et al. Use of Massage Therapy for Pain, 2018-2023: A Systematic Review. JAMA Network Open. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11250267/
Acupuncture vs Usual Care for Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Immediate and Intermediate Effects. PMC. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12867475/
Li X, et al. Comparative Efficacy of Acupuncture for Chronic Low Back Pain: A Network Meta-Analysis. Heliyon. 2025. https://www.cell.com/heliyon/fulltext/S2405-8440(25)01513-0
Zhang Z, et al. The effectiveness of cupping therapy on low back pain: A systematic review and meta-analysis of randomized control trials. Complementary Therapies in Medicine. 2024;80:103013. https://www.sciencedirect.com/science/article/pii/S0965229924000013
Sciatica: References
National Institute for Health and Care Excellence (NICE). Low Back Pain and Sciatica in Over 16s: Assessment and Management. NICE Guideline [NG59]. Published November 2016, last updated December 2020. https://www.nice.org.uk/guidance/ng59
Peene L, et al. Lumbosacral radicular pain. Pain Practice. 2024;24(3):471-483. https://onlinelibrary.wiley.com/doi/10.1111/papr.13317
Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ. 2007;334(7607):1313-1317. https://pmc.ncbi.nlm.nih.gov/articles/PMC1895638/
Stoker GE, et al. Musculoskeletal mimics of lumbosacral radiculopathy. Muscle and Nerve. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11998970/
Kaly. How Long Does Sciatica Nerve Pain Last? 2023. https://www.kaly.com/blog/how-long-does-sciatica-nerve-pain-last/
Effectiveness of Nonsurgical Interventions for Patients With Acute and Subacute Sciatica: A Systematic Review With Network Meta-Analysis. Journal of Orthopaedic and Sports Physical Therapy. 2025. https://www.jospt.org/doi/10.2519/jospt.2025.13068
Kuligowski T, Skrzek A, Cieslik B. Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2021;18(11):6176. https://pmc.ncbi.nlm.nih.gov/articles/PMC8201115/
Neural Mobilization for Reducing Pain and Disability in Patients with Lumbar Radiculopathy: A Systematic Review and Meta-Analysis. PMC. 2023. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10744707/
Qu Z, Ju J, Qin H, Ding Y, Peng L. Effectiveness of acupuncture in the treatment of chronic sciatica from herniated disks: a systematic review and meta-analysis. Frontiers in Medicine. 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12872920/
Zhang Z, et al. The effectiveness of cupping therapy on low back pain: A systematic review and meta-analysis of randomized control trials. Complementary Therapies in Medicine. 2024;80:103013. https://www.sciencedirect.com/science/article/pii/S0965229924000013
Du X, et al. Clinical efficacy of exercise therapy for lumbar disc herniation: a systematic review and meta-analysis of randomized controlled trials. Frontiers in Medicine. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11985520/
Yu P, et al. Characteristics and mechanisms of resorption in lumbar disc herniation. Arthritis Research and Therapy. 2022;24:205. https://d-nb.info/1272592871/34
The Diagnosis and Treatment of Degenerative Changes of the Lumbar Spine. PMC. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12516344/
Kim KH, et al. Facet joint disorders: from diagnosis to treatment. Korean Journal of Pain. 2024;37(1):1-15. https://pmc.ncbi.nlm.nih.gov/articles/PMC10764212/
Piazza S, et al. Piriformis syndrome: a systematic review of case reports. BMC Surgery. 2025;25:468. https://pmc.ncbi.nlm.nih.gov/articles/PMC12512919/
Those are ready to copy and paste directly into your blog. A couple of things worth noting:
Reference 5 in the sciatica blog pulls together data from multiple recovery timeline sources — if you would like me to expand this into two or three separate references for each claim, I can do that.
Reference 12 links to a German National Library copy of the Arthritis Research and Therapy paper — if you would prefer, I can find the direct PubMed link for that one.



Comments