
What Headache Do I Have? Cervicogenic, Migraine, or TMD?
- staystrongtherapy
- Jun 30
- 16 min read
Updated: Jul 4
All information in this blog is supported by peer-reviewed research. Reference numbers appear throughout, with the full list at the bottom of the page.
The Headache That's Hard to Pin Down
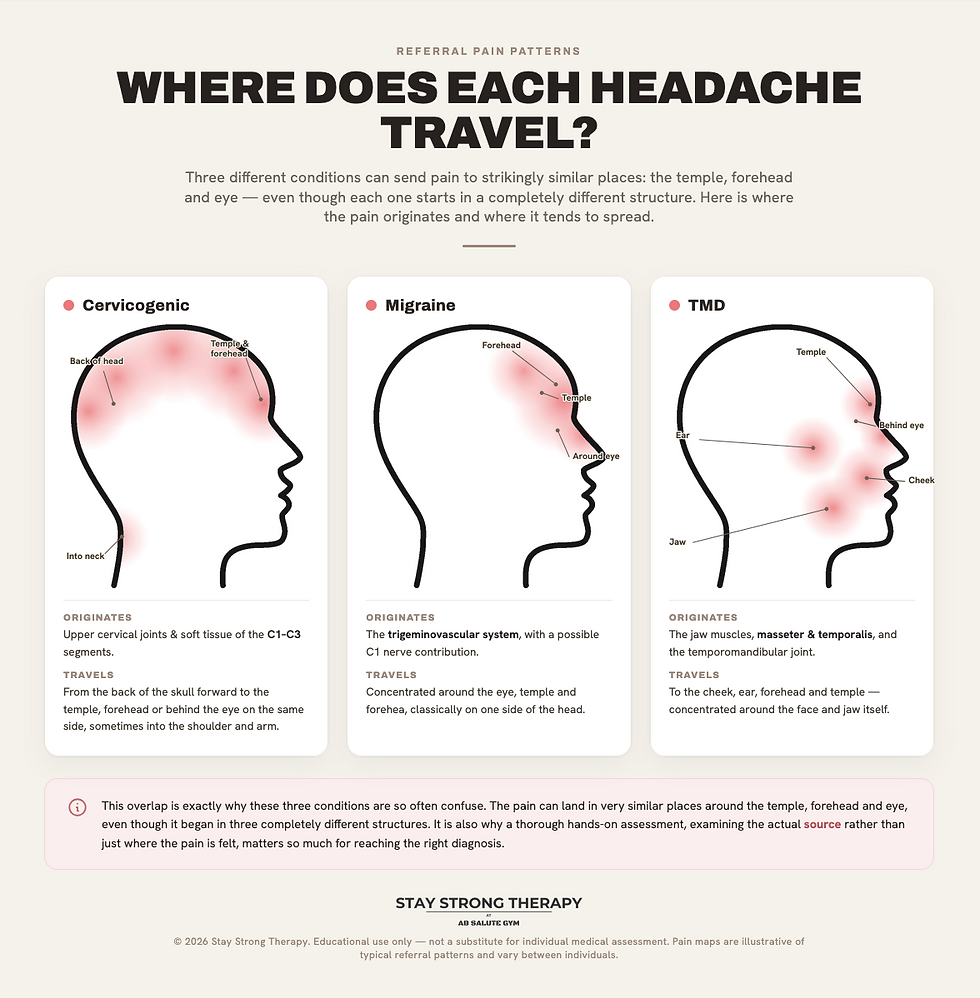
Cervicogenic headache, migraine, and temporomandibular disorder (TMD) related headache share clinical overlap that even experienced clinicians find them difficult to tell apart without a thorough, structured assessment. Research has found that within groups of people diagnosed with migraine or tension-type headache, a meaningful proportion actually meet the diagnostic criteria for cervicogenic headache once properly assessed. ¹
This blog is designed to help you understand the key differences between these three conditions, why they get confused so often, and what we can do to help.
Tension type headaches blog can be found here.
What Is a Cervicogenic Headache?
A cervicogenic headache is a headache that originates from a problem in the cervical spine, the neck, rather than from the brain itself. It is what is known as a secondary headache: the pain is a symptom of an underlying musculoskeletal issue, most commonly involving the upper cervical joints (particularly the C1 to C3 segments), the surrounding muscles, or the nerves that supply this region. ²
The reason neck problems can cause headache pain lies in the anatomy. The upper cervical nerves and the trigeminal nerve, which supplies sensation to the face and head, converge within the same area of the spinal cord known as the trigeminocervical nucleus. Because these pain signals essentially merge at this junction, pain originating in the neck can be perceived by the brain as coming from the head, a phenomenon known as referred pain. ²
Diagnostic criteria for cervicogenic headache include: ³
Headache that develops in close relation to the onset of a neck problem, or an existing neck condition
Headache that significantly improves or resolves alongside improvement in the underlying neck condition
Reduced cervical range of motion, with headache significantly provoked by neck movements or sustained postures
Headache that is substantially relieved following a diagnostic nerve block to a cervical structure (used in clinical research, less commonly in routine practice)
Research has found that a specific combination of findings, including reduced cervical movement, signs at the upper cervical joints, and impaired deep neck flexor muscle function, accurately identifies cervicogenic headache and reliably differentiates it from migraine and tension-type headache when assessed together. ⁴ This is exactly why a thorough hands-on assessment matters so much for getting the right diagnosis.
Common Signs and Symptoms of Cervicogenic Headache
Headache that is almost always one-sided, and stays on the same side with each episode
Pain that starts at the back of the head or neck and spreads forward toward the forehead, temple, or behind the eye
Reduced neck range of motion, particularly with rotation
Headache brought on or worsened by sustained neck postures, certain neck movements, or pressure over the upper neck
Associated neck stiffness or tenderness, often most pronounced at the base of the skull
Headaches that tend to be moderate in intensity rather than severe, and are typically not associated with nausea, vomiting, or visual disturbance, although mild versions of these can occasionally occur
A gradual, often less dramatic onset compared with migraine
Cervicogenic headache also has a notably different demographic pattern compared to the headache conditions it is often confused with. Research has found that the average age at diagnosis is around 43 years, with a strong female predominance of around 4 to 1. ⁵ This fits closely with the same midlife pattern discussed in our neck pain and stiffness blog, where loss of thoracic compliance and increased cervical compensation often begin to surface as new symptoms in the late 30s and 40s.
How Is Cervicogenic Headache Different From Migraine?
This is one of the most common points of confusion, and the overlap is genuinely significant. Both conditions can be one-sided, both can be triggered or worsened by neck movement or posture, and both can be associated with neck pain. Research has found that neck pain is reported by a substantial proportion of people with migraine, which is part of why the two are so often mixed up. ⁶
However, there are several useful distinguishing features:
Feature | Cervicogenic Headache | Migraine |
Side of pain | Always the same side | Can switch sides between episodes |
Onset | Gradual, often related to neck position or movement | Can be more sudden, with or without warning (aura) |
Triggered by | Specific neck movements or sustained postures | Hormonal changes, certain foods, stress, sleep disruption, light or sound |
Associated nausea/vomiting | Uncommon | Common, sometimes severe |
Light and sound sensitivity | Uncommon or mild | Common, often pronounced |
Visual disturbance (aura) | Not a feature | Can occur before or during the headache |
Neck restriction on examination | Present and measurable | Often normal or only mildly restricted |
Response to neck treatment | Headache improves alongside neck improvement | Typically does not resolve with neck treatment alone |
A particularly useful clinical clue is the flexion-rotation test, a hands-on assessment of upper cervical rotation performed with the neck fully flexed. Restricted movement on this specific test is strongly associated with cervicogenic headache and has been validated against diagnostic nerve blocks as part of an accurate diagnostic pattern. ⁴
It is also worth knowing that the two conditions are not always mutually exclusive. Some people experience both migraine and cervicogenic headache, and neck dysfunction can act as a genuine trigger for migraine episodes in people who are migraine-prone, even though the underlying mechanisms of the two conditions are different. ⁶
How Is Cervicogenic Headache Different From TMD Related Headache?
This is the other major area of overlap, and the relationship between the neck and the jaw is closer than most people realise. The temporomandibular joint, the jaw joint, sits very close to the upper cervical spine, and research has consistently found a strong clinical association between the two. People with neck pain or cervicogenic headache show significantly higher rates of TMD, reduced jaw mobility, increased jaw muscle tenderness, and more temporomandibular trigger points compared to people without these conditions. ⁷ The relationship runs both ways too, with people who have painful TMD showing notably higher odds of also having cervicogenic headache. ⁸
This overlap exists because the trigeminal nerve, which supplies the jaw and face, and the upper cervical nerves, converge in the same area of the brainstem described earlier. Dysfunction in one area can therefore directly influence pain perception in the other, and chronic tension or restriction in one region frequently develops alongside problems in the other.
Key differences to look out for:
Feature | Cervicogenic Headache | TMD Related Headache |
Primary location | Base of skull, spreading to forehead or temple | Temple, jaw, ear, or face, sometimes spreading to the head |
Jaw symptoms | Usually absent or secondary | Jaw clicking, locking, pain with chewing, or restricted jaw opening |
Worsened by | Neck movement or sustained neck postures | Chewing, yawning, clenching, or jaw movement |
Neck range of motion | Reduced | Can be normal, although often also reduced if both conditions coexist |
Jaw range of motion | Usually normal | Often reduced |
Associated history | Neck strain, whiplash, postural strain | Teeth grinding (bruxism), jaw clenching, dental work, stress |
Because TMD and cervicogenic headache so frequently coexist, a thorough assessment of both the neck and the jaw is genuinely important. Treating the neck alone in someone whose headache is being driven primarily by TMD, or vice versa, will likely lead to incomplete or short-lived improvement.
Why Does the Confusion Matter?
Beyond simple curiosity, getting an accurate picture of which condition, or combination of conditions, is driving your headaches matters because the treatment approaches differ. Migraine often requires medical management alongside lifestyle and trigger identification. TMD related headache requires assessment and treatment of the jaw, sometimes alongside dental or orthodontic input. Cervicogenic headache, by contrast, responds specifically to treatment directed at the neck.
This is why a proper hands-on assessment, rather than guesswork or self-diagnosis from internet searching, is so valuable. Research evaluating the diagnostic criteria for cervicogenic headache has repeatedly found that no single sign or symptom is reliable enough in isolation: it is the specific combination and pattern of findings on examination that allows for an accurate diagnosis. ⁹
When Should You Be Concerned? Red Flags to Watch For
The vast majority of headaches, including all three conditions discussed here, are benign. However, certain features require urgent medical assessment:
A sudden, severe "thunderclap" headache reaching maximum intensity within seconds to minutes
Headache with fever, neck stiffness, confusion, or a non-blanching rash
Headache following significant head or neck trauma
New headache with progressive weakness, numbness, visual loss, slurred speech, or loss of balance
A new headache pattern in someone over 50 with no previous history of headaches
Headache that wakes you from sleep, or is significantly worse first thing in the morning, accompanied by vomiting
Unexplained weight loss alongside persistent headache
If you experience any of these, please seek prompt medical attention before pursuing manual therapy treatment.
How We Can Help With Cervicogenic Headache
Once a cervicogenic origin, or a significant cervical contribution to your headaches, has been identified through thorough assessment, the evidence for manual therapy treatment is genuinely strong.
Osteopathic manual techniques and cervical spine mobilisation: Research evaluating manual therapy specifically for cervicogenic headache has found that the most effective interventions combine techniques targeting the upper cervical segments, particularly C1 to C2 and C3, alongside soft tissue work and exercise. ¹⁰ A comparative trial of different manual therapy approaches found meaningful improvements in headache frequency, pain intensity, and disability following spinal manipulation and mobilisation techniques targeting the upper neck. ¹¹ Further research comparing spinal manipulation, mobilisation, and massage for cervicogenic headache further supports manual therapy as an effective management approach. ¹²
Spinal mobilisation and gentle manipulation: Techniques such as sustained natural apophyseal glides, a specific gentle mobilisation technique applied to the upper cervical joints, have shown good evidence for reducing both headache frequency and intensity in people with cervicogenic headache. ¹³
Deep tissue and sports massage: Research has found that targeted soft tissue techniques, particularly addressing the upper trapezius and sternocleidomastoid muscles, provide effective short-term relief of cervicogenic headache symptoms, and work particularly well when combined with joint-focused manual therapy for longer-lasting results. ¹⁰
Medical acupuncture:Used as part of a broader treatment plan, medical acupuncture can help address the chronic muscle tension and trigger points in the upper trapezius, sternocleidomastoid, and suboccipital muscles that frequently accompany cervicogenic headache, alongside reducing overall pain sensitivity.
Cupping and gua sha: Effective complementary tools for releasing persistent tension in the upper neck and shoulder muscles that often contributes to ongoing cervicogenic symptoms.
Combined manual therapy and exercise: The strongest evidence consistently points toward combining manual therapy with targeted exercise rather than using either approach alone. Research comparing combined manual therapy and exercise against exercise alone found that the combined approach produced significantly better outcomes in headache intensity, disability, and cervical movement, both in the short term and over several months of follow up. ¹⁴
Exercise for Cervicogenic Headache
Exercise plays a genuinely important role in long-term management, particularly given that people with cervicogenic headache have been shown to have weaker deep neck flexor muscles compared to people with other headache types, with this weakness compensated for by increased tension in the more superficial neck muscles. ¹⁰
Deep neck flexor activation
Chin tucks (craniocervical flexion): lying on your back or sitting upright, gently nod the chin in a small "yes" motion, drawing the head straight back without tilting it downward. Hold for 5 to 10 seconds, repeat 10 times. This specific exercise, often guided initially with feedback from a practitioner, directly targets the deep neck flexor weakness identified in cervicogenic headache. ¹⁰
Upper cervical mobility
Gentle chin nods through range: small, controlled nodding movements at the very top of the neck, distinct from full neck flexion, to gently restore mobility at the C1 and C2 segments most commonly implicated in cervicogenic headache.
Soft tissue release
Upper trapezius stretch: sitting upright, gently tilt one ear toward the same shoulder, using the opposite hand for light overpressure. Hold 30 seconds each side.
Suboccipital release: lying on your back with a small towel roll or soft ball placed at the base of the skull, gently resting the head's weight onto it for 1 to 2 minutes to release tension in the muscles connecting the skull to the upper neck.
Postural support
Doorway chest stretch: standing in a doorway with arms at 90 degrees, lean gently forward until a stretch is felt across the chest, reducing the forward head posture that places additional strain on the upper cervical joints.
Thoracic rotation exercises: as discussed in our neck pain and stiffness blog, restoring thoracic spine mobility reduces the compensatory load placed on the upper cervical spine, addressing one of the underlying contributors to cervicogenic headache.
Research evaluating the effectiveness of exercise alone, without manual therapy support, found that a deep neck flexor exercise programme on its own may not be the most appropriate approach for this condition: combining the exercise programme with manual therapy produced significantly better results across headache intensity, disability, and cervical movement measures. ¹⁴ This is why we always pair exercise prescription with hands-on treatment for cervicogenic headache, rather than relying on exercise in isolation.
How We Can Help With Migraine
Whilst migraine itself is a neurological condition requiring medical management as the primary approach, manual therapy can play a genuinely useful supporting role, particularly in people whose migraine attacks are linked to or worsened by neck dysfunction.
Research has found that neck-related musculoskeletal impairment is common in people with migraine, and addressing this component can meaningfully reduce overall headache burden even though it does not treat the underlying migraine mechanism itself. ¹⁵ A randomised controlled trial comparing manual therapy plus usual care against usual care alone in people with migraine and coexisting neck pain found that manual therapy provided a useful adjunctive benefit, supporting its use alongside, rather than instead of, standard migraine management. ¹⁶
A three-armed trial combining manual therapy, neck muscle exercise, and pain education found that all approaches led to improvement over time, with the combined multimodal approach showing the most consistent benefit at longer-term follow up. ¹⁷ Separate research comparing connective tissue massage with manual lymphatic drainage in migraine patients found that manual lymphatic drainage had a stronger effect on overall pain relief and wellbeing, whilst connective tissue massage was particularly effective for reducing the coexisting neck pain and disability that so commonly accompanies migraine. ¹⁸
Manual therapy and massage: Gentle soft tissue work targeting the neck and shoulder muscles, alongside connective tissue massage techniques, can help reduce the neck-related component that frequently accompanies and can trigger migraine attacks.
Medical acupuncture: Used alongside standard migraine management, acupuncture can help address coexisting muscle tension and pain sensitivity, supporting overall symptom management.
Exercise for Migraine
Gentle neck mobility and deep neck flexor exercises: the same chin tuck exercise described in the cervicogenic headache section can help address coexisting neck dysfunction, which research has shown to be common in people with migraine. ¹⁵
Regular aerobic activity: research into physical activity and migraine has found a clear relationship between activity levels and improvements in pain, function, and quality of life, making gentle, consistent exercise a genuinely useful part of overall migraine management. ¹⁹
Postural and shoulder release work: stretches such as the doorway chest stretch and upper trapezius stretch described above can help reduce the secondary muscular tension that frequently builds up around migraine episodes.
It is important to be clear that manual therapy and exercise are a supportive, adjunctive approach for migraine, not a replacement for appropriate medical management. We would always encourage ongoing communication with your GP or neurologist regarding your migraine treatment plan.
How We Can Help With TMD Related Headache
Where the jaw is identified as a significant contributor to your headaches, treatment specifically targeting the temporomandibular joint and surrounding structures has good supporting evidence.
Research evaluating a multimodal physical therapy approach for TMD found that combining structured manual therapy with craniomandibular stabilisation exercise produced significant reductions in pain alongside meaningful improvements in jaw function and muscle tenderness. ²⁰ Research specifically evaluating joint mobilisation for TMD found consistent improvements across pain intensity, jaw range of motion, and muscle activity outcomes. ²¹
Given how closely TMD and cervicogenic headache are linked, the evidence also supports treating the neck alongside the jaw. A randomised controlled trial comparing neck-specific exercise, manual therapy, and a placebo group in women with chronic TMD found that targeted neck exercise produced meaningful improvements in orofacial pain, jaw function, and quality of life, supporting the cervical spine as a genuine and worthwhile treatment target in TMD, not just the jaw itself. ²²
Jaw and craniomandibular manual therapy: Hands-on mobilisation and soft tissue release of the jaw muscles and temporomandibular joint, working alongside cervical treatment where the neck and jaw are both contributing to symptoms.
Cervical and masticatory soft tissue release: Research has found that combined soft tissue release targeting both the neck and the jaw muscles, delivered as part of a broader treatment programme, produced meaningful improvement in TMD related symptoms. ²³
Exercise for TMD
Jaw range of motion exercises: gentle, controlled opening and closing of the jaw within a comfortable range, performed slowly and without forcing, to maintain and gradually improve mobility.
Jaw stabilisation exercises: gentle resisted opening, closing, and lateral movements performed with light fingertip resistance, building control and reducing excessive joint movement during chewing and speaking.
Neck motor control and deep neck flexor training: given the strong evidence linking neck dysfunction to TMD, the same chin tuck and deep neck flexor exercises described for cervicogenic headache form a genuinely useful part of TMD management, with research showing meaningful improvement in orofacial pain and jaw function from neck-focused exercise alone. ²²
Postural exercises: forward head posture places the jaw in an altered resting position, increasing strain on the temporomandibular joint, so the same thoracic and postural exercises described earlier in this blog are relevant here too.
Relaxation and awareness of jaw clenching: given the close relationship between stress, bruxism (teeth grinding), and TMD symptoms, gentle awareness exercises to notice and release unconscious jaw clenching throughout the day can meaningfully reduce symptom frequency.
If dental factors such as bruxism or bite alignment appear to be significant contributors to your TMD, we would also recommend liaising with your dentist, as a combined approach addressing both the musculoskeletal and dental aspects tends to produce the best long-term outcomes.
Living With Headaches: Practical Day-to-Day Tips
Workstation setup: screen at eye level, with attention to avoiding sustained neck rotation or prolonged downward gaze, both common triggers for cervicogenic symptoms.
Phone use: bring the phone to eye level rather than tilting the head down, particularly during long periods of use.
Sleeping position and pillow: a pillow that maintains a neutral neck position, avoiding excessive flexion or extension overnight, can meaningfully reduce morning headache frequency.
Movement breaks: regular gentle neck and thoracic movement throughout the day helps prevent the sustained postures that commonly trigger cervicogenic headache.
Track your pattern: keeping a simple headache diary noting side, triggers, associated jaw or neck symptoms, and response to movement can be genuinely useful for both your own understanding and for guiding treatment, regardless of which condition you have.
Stress and jaw tension: given the close relationship between TMD and cervicogenic headache, being mindful of jaw clenching, particularly during stressful periods or sleep, can help reduce overlap between the two conditions.
Migraine triggers: if migraine is part of the picture, tracking sleep, hydration, food, and hormonal patterns alongside your headache diary can help identify personal triggers worth discussing with your GP.
What to Expect at Your First Appointment
At your first appointment, we will take a thorough headache history, including the location, pattern, triggers, and associated symptoms of your headaches, alongside specific questions designed to help distinguish between cervicogenic headache, migraine, and TMD related presentations. We will carry out a hands-on assessment of your upper cervical spine, including specific tests such as the flexion-rotation test, alongside an assessment of your jaw if relevant. We will explain clearly what we find and, where appropriate, advise on referral for further medical assessment if your presentation suggests migraine or another primary headache disorder requiring a different treatment approach.
Frequently Asked Questions
Can I have more than one type of headache at once? Yes, this is genuinely common. Many people have a combination of cervicogenic features alongside migraine or TMD, and addressing the cervical component can often reduce overall headache burden even when it isn't the sole cause.
Will treating my neck definitely stop my headaches? If your headaches are genuinely cervicogenic in origin, treatment directed at the neck typically produces meaningful improvement. If migraine or TMD is the primary driver, neck treatment may provide some benefit but is unlikely to fully resolve symptoms without also addressing the primary condition.
How long will treatment take? Research suggests that one to two manual therapy sessions per week for around six weeks tends to produce the best outcomes for cervicogenic headache, with more frequent sessions not necessarily producing faster or greater improvement. ¹⁰ Many people notice a meaningful reduction in headache frequency within the first few weeks of combined manual therapy and exercise.
Do I need a scan? In most cases, no. Cervicogenic headache is diagnosed through history and clinical examination. Your practitioner will advise if imaging or referral is appropriate based on your specific presentation, particularly if any red flag features are present.
What if my headache turns out to be migraine? We will be upfront about this during your assessment. We can still support you with the neck-related component of your symptoms, but we will also encourage you to discuss appropriate medical management with your GP or neurologist.
Not sure which type of headache you're dealing with? Get in touch using the contact form and we will carry out a thorough assessment to help identify exactly what's going on and the right treatment approach for you.
References
Cervicogenic headache: a critical review of the current diagnostic criteria. Cephalalgia. 1998. Available at: https://www.sciencedirect.com/science/article/abs/pii/S030439599800116X
Cervicogenic headache and occipital neuralgia. Pain Practice. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11680101/
Sustained Natural Apophyseal Glide and Deep Friction Massage in Patients With Cervicogenic Headache, ICHD-III Diagnostic Criteria. ClinicalTrials.gov. Available at: https://clinicaltrials.gov/study/NCT05404113
Cervicogenic headache, an easy diagnosis? A review of diagnostic studies. Musculoskeletal Science and Practice. Available at: https://www.sciencedirect.com/science/article/abs/pii/S2468781222001400
Cervicogenic headache: a critical review of the current diagnostic criteria. PubMed. Available at: https://pubmed.ncbi.nlm.nih.gov/9822206/
Ashina S, Bendtsen L, Lyngberg AC, et al. Prevalence of Neck Pain in Migraine and Tension-Type Headache: A Population Study. Cephalalgia. 2015;35(3):211-9. Referenced via: https://www.binasss.sa.cr/bibliotecas/bhm/may24/36.pdf
Temporomandibular Disorders and Orofacial Outcomes in Subjects with Neck Pain and/or Cervicogenic Headache. Journal of Clinical Medicine. 2025. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12786625/
The association between specific temporomandibular disorders and cervicogenic headache. PubMed. Available at: https://pubmed.ncbi.nlm.nih.gov/33482538/
Demont A, Lafrance S, Benaissa L, Mawet J. Cervicogenic headache, an easy diagnosis? Diagnostic studies overview. Musculoskeletal Science and Practice. 2022;62:102640.
Núñez-Cabaleiro P, Leirós-Rodríguez R. Effectiveness of manual therapy in the treatment of cervicogenic headache. Headache: The Journal of Head and Face Pain. 2022;62(3):271-283. Available at: https://headachejournal.onlinelibrary.wiley.com/doi/10.1111/head.14278
Comparative Effects of Mulligan's Mobilization, Spinal Manipulation, and Conventional Massage Therapy in Cervicogenic Headache. PMC. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9819355/
Xu X, Ling Y. Comparative safety and efficacy of manual therapy interventions for cervicogenic headache. Frontiers in Neurology. 2025. Available at: https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2025.1566764/full
Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K. Efficacy of a C1-C2 self-sustained natural apophyseal glide (SNAG) in the management of cervicogenic headache. Journal of Orthopaedic and Sports Physical Therapy. 2007;37:100-7.
Short and medium-term effects of manual therapy on the upper cervical spine combined with exercise vs isolated exercise in patients with cervicogenic headache. Musculoskeletal Science and Practice. Available at: https://www.sciencedirect.com/science/article/abs/pii/S1746068922000219
Pensri C, Liang Z, Treleaven J, et al. Cervical musculoskeletal impairments in migraine and tension-type headache and relationship to pain related factors. Musculoskeletal Science and Practice. 2025;76:103251.
Effectiveness of manual therapy as a prophylactic treatment for migraine: a randomized controlled trial. Archives of Physiotherapy. Available at: https://www.archivesofphysiotherapy.com/index.php/aop/article/view/3799
Effects of combining manual therapies, neck muscle exercises, and therapeutic education pain neuroscience in patients with migraine. Musculoskeletal Science and Practice. Available at: https://www.sciencedirect.com/science/article/abs/pii/S2468781225001080
Comparison of the efficacy of connective tissue massage and manual lymphatic drainage in patients with migraine: a randomized controlled trial. Journal of Oral and Facial Pain and Headache. 2025;39(3):121-132.
Sağlı Diren G, Kaya Ciddi P, Ergezen G, Şahin M. Effect of physical activity level on pain, functionality, and quality of life in migraine patients. The Journal of the Turkish Society of Algology. 2023;35:212.
Multimodal physical therapy approach for the management of patients with temporomandibular disorder: Randomized control trial. PMC. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11951998/
The effectiveness of mobilization in treating patients with temporomandibular disorders. PMC. 2025. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC12481914/
de Oliveira-Souza AIS, et al. Effectiveness of an 8-week neck exercise training on pain, jaw function, and oral health-related quality of life in women with chronic temporomandibular disorders. Journal of Oral and Facial Pain and Headache. 2024;38(1):40-51.
The effectiveness of conservative interventions on temporomandibular disorder-related kinesiophobia and pain catastrophizing. Musculoskeletal Science and Practice. 2025.



Comments